Now is the time to listen to uncomfortable truths
The importance of listening to the lived experienced “behind the numbers” when reviewing the disproportionate numbers deaths of Black Minority and Ethnic communities from Covid-19.

In this post, I’ll explore the idea that we need a different approach in trying to understand the disproportionate number of BAME deaths from Covid-19 in the UK. Rather than just trying to identify the risk factors that lead to the increased rate of Covid-19 cases of critical illness and deaths for BAME ethnic groups, any review into reasons behind the disproportionate effects on BAME communities must go further to understand the lived experience of real people from BAME communities.
When considering data on numbers of critically ill or numbers of deaths, it’s important to remember that each statistic of a death is a real person: whether a mother, a son, a father and in all cases a member of a community. I’ll put forward the idea that a concept that can help us to consider the complexity of lived experience, intersectionality.
Finally, I’ll point towards a new campaign that has been advanced by by high- level leaders from BAME communities on this particular issue. This is the #weneedanswers campaign.
To start off, let’s recap the problem.
The effect on BAME communities is starkly disproportionate
Statistics on the numbers of hospital deaths from the Institute of Fiscal Studies (IFS) suggested that “Other Ethnic Groups” were at greatest risk of in-hospital deaths (80 deaths per 100,000 people). People of Caribbean descent was the second most affected category (78 deaths per 100,000 people). In contrast, the data found only 27 deaths per 100,000 for the white British category. This contrast is even more stark given that Black Minority and Ethnic individuals comprise only 14% of the total UK population.
Ross Warwick, a research economist at IFS and co-author of the report said:
“There is unlikely to be a single explanation here and different factors may be more important for different groups. For instance, while black Africans are particularly likely to be employed in key worker roles which might put them at risk, older Bangladeshis appear vulnerable on the basis of underlying health conditions.”
In terms of NHS staff, 44 per cent of NHS doctors are from a BAME background and 24 per cent of NHS nurses are from BAME communities. The first doctor to lose their life to Covid-19 was 76-year-old GP Dr Habib Zaidi, who tragically died on 25 March this year. NHS health care workers of Filipino descent have also been disproportionately affected by Covid-19.
PPE provision is another factor affecting NHS workers
There have been cases of NHS workers who were reported as not being provided with adequate personal protective equipment. A notable case was that of Thomas Harvey, a 57 year old health care assistant who was given gloves but not adequate Personal Protective Equipment and sadly died.

More research is needed to understand why BAME communities have been hit
There is widespread agreement that further research is needed to understand the causes of the greater risk of critical illness and death for Black and Minority Ethnic communities. In a report in Nursing Times experts suggest a national inquiry is needed.
“It is essential to tackle the underlying social and economic risk factors that lead to these unjust deaths” -Delan Devakumar, Associate Professor in Child and Adolescent Health, Institute of Child Health, University College London.
In response to the increased risk, a review has been launched by Public Health England to explore the reasons for the disproportionate impact on Black and Minority Ethnic communities. The review will be led by Trevor Phillips. There has also been calls to capture ethnicity data in hospitals and the issue has been described as an urgent public health priority.
Some risk factors are already known
Many reasons that are specific to different Black and Minority Ethnic communities have been proposed already. Some factors relate to underlying health conditions that have a higher prevalence in specific Black and Minority Ethnic communities. For example, more people have high blood pressure of Afro Caribbean descent that can put this community at increased risk. The increased prevalence of diabetes for South Asians has been put forward as another risk factor. Increased exposure due to working on the front lines as public transport workers and working with patients and those that are at risk provide more reasons. Researchers from the Kings Fund have written:
However, these risk factors can tell us about an increased likelihood, they do not necessarily show all the pieces of the puzzle that have caused to the increased cases and deaths to Black and Minority Ethnic communities.
In addition to identifying risk factors that link with greater risk of exposure and death, it is important to consider lived experience of individuals from Black and Minority Ethnic communities. The notion of intersectionality is relevant here.
What is intersectionality?
Intersectionality was the brain child of Columbia University law professor and activist Kimberlé Williams Crenshaw. In her widely acclaimed paper, Mapping the Margins, she argued (drawing on her earlier writing):
“I used the concept of intersectionality to denote the various ways in which race and gender interact to shape the multiple dimensions of Black women’s employment experiences. My objective there was to illustrate that many of the experiences Black women face are not subsumed within the traditional boundaries of race or gender discrimination as these boundaries are currently understood, and that the intersection of racism and sexism factors into Black women’s lives in ways that cannot be captured wholly by looking at the race or gender dimensions of those experiences separately.
As a researcher of the law, Crenshaw noticed that there was a lack of language to speak about how the specific experiences of black women differed from black men, or from white women. Laws designed to protect black men did not protect black women, and laws to protect white women did not protect black women, either. Thus, gender and racial discrimination was intersecting for women of colour.
In other words, rather than the effects of racism or sexism operating in isolation, to truly understand their effects on people, it is important to understand the total impact of unequal social structures on the individual and how they may collide.
Crenshaw explains the concept herself in this video suggesting that intersectionality is a metaphor for the way that multiple forms of disadvantage compound themselves. She points to the fact that in the US African American girls are six times more likely to be expelled from high school than their white counterparts.
Intersectionality is not only about race and gender, it relates to all aspects of social identities: class, socio-economic status, religion, sexuality, able bodied versus having a disability. Writer and speaker Ijeoma Oluo explains:
“Each of us has a myriad of identities- our gender, class, race, sexuality and so much more, that inform our experiences in life and our interactions out in the world….These privileges and oppressions do not exist in a vacuum, however, they can combine with other, mitigate each other and contradict each other” (p. 75)
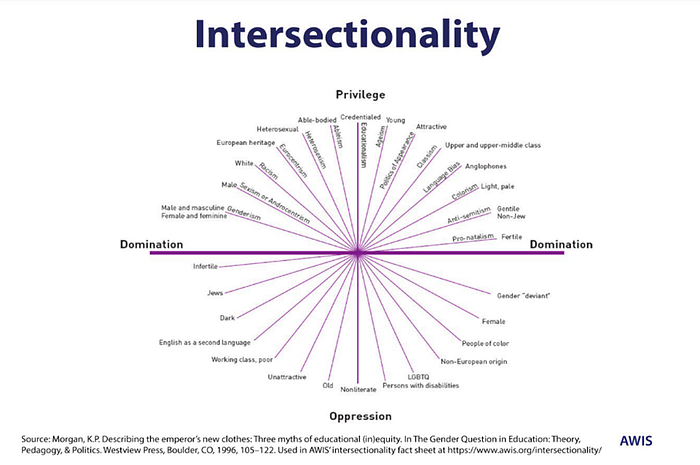
Good ideas travel. The idea of intersectionality has traveled across the fields of law, sociology, psychology, education and more. The diagram below shows the multiple ways that different levels of privileged intersect with all aspects of identities.
Within psychology, the American Psychological Association (APA) encourages psychologists to be sensitive to intersectionality, they define it as:
“the way in which individuals are shaped by and identify with a vast array of cultural, structural, sociobiological, economic, and social contexts (Howard & Renfrow, 2014).”
APA brings attention to the fact that structural inequalities can be a driver of marginalised identities. All too often reviews, public inquiries, reports present research on risk factors but scholarship does not consider issues of intersectionality despite being recommended by trusted bodies such as APA.
In understanding the disproportionate number of BAME deaths from Covid-19, considering intersectionality is crucial. It’s key not to just to consider risk factors such as underlying health conditions, but how multiple factors may intersect and exert cumulative effects. Further, what structural factors may contribute to risk of particular health conditions? For example, for low paid workers, what educational opportunities led to the job undertaken, what other caring constraints did an individual face?
It’s important to examine the cumulative effect of intersecting risk factors on individuals and aspects of social identities.
Instead of talking only about race and health outcomes, it is important to talk about racism and the social determinants of vulnerability. Understanding what being at increased risk as a minority means to those who experience it, is important. Issues of poverty, racism, and discrimination need to be explored as well. It is important not only to look at quantitative data but to explore the subjective experiences of individuals from BAME communities and the lived experience of risk factors.
Some years back, I have had the privilege to work with Yvonne Field, founder of the Ubele Initiative, a respected leader in the African and Caribbean community in the UK, an academic and an all-round remarkable person. Ubele means “the future” in Swahili and a concern for the future of the African diaspora is part of the fabric of the organisation. Ubele’s mission is to contribute to the sustainability of the African Diaspora community.
Ubele is currently asking the Government for a full independent public inquiry into deaths from Covid-19 from a an ethnic minority background as published by the BBC today. There is an open letter on their website (link here) that has been live from today the 10th May, 2020.
It is important that there is space for leadership comes from BAME communities that is driven by leaders from BAME communities. I am white. I have a mixed race child. I know that I can not speak on behalf of or for BAME communities because I’m a white woman. I am increasingly coming to understand that I may not ever fully know what it feels like to be a person of colour. I’ve learned from reading Ijeoma Oluo that my skin colour is a barrier to me having total empathy with someone who belongs to a minority group. In her book, So You Want To Talk About Race, Oluo reminds white people about some tips about talking about race:
“You are not living as a person of colour. You will never fully understand the impact that sustained systemic racism has on people of colour.”

It is true that white people may never fully understand the impact of sustained systemic racism on people of colour. But white people can try and understand and develop a deeper understanding. We can stop only talking about statistics and consider what the experience of an increased rate of deaths might look and feel like. We can shift from an attitude of “tolerance” to an attitude of “hospitality” to welcoming understanding lived experience and understanding difference.
Given that in the UK (and in America) the death rate for BAME communities is more than twice that of whites it is a prescient time to talk and listen about the experience of race and racism and understand difference.
Finally, a note of optimism. Perhaps the present inquiries into BAME deaths for Covid-19 have the potential to be be part of a larger process of understanding the impact of sustained systemic racism and the lived experience of racial and socioeconomic inequalities. It is essential to overcome racism and discrimination in the UK. Some light at the end of the Covid-19 tunnel is an opportunity for British society to overcome racism and shed light on the structural inequalities that lead to tragic and unjust differences in outcomes.
This work is licensed under a Creative Commons Attribution-NoDerivatives 4.0 International License.
